If this is your first pregnancy or child, you may or may not have heard about “Diastasis Recti” or ab separation that happens during and can last after pregnancy. It’s a condition that actually affects most mothers, but many women are unaware of the possibility of having lasting ab separation after pregnancy. Not all doctors will routinely discuss ab separation after pregnancy (neither my doctor or midwives assessed me for diastasis recti after my pregnancies). Therefore, its a good idea to be proactive and learn how to check for ab separation after pregnancy, before you start exercising again. Its important to understand how it can affect your body and how you should move and exercise in the postpartum period if you have ab separation.
In this post, I will provide an overview of diastasis recti, I will review the latest clinical research on diastasis recti, and with the help of my good friend Jen Hodgkinson, a pilates and movement teacher as well as postnatal exercise specialist, describe how you can check your own abs for separation.
What is Diastasis Recti?
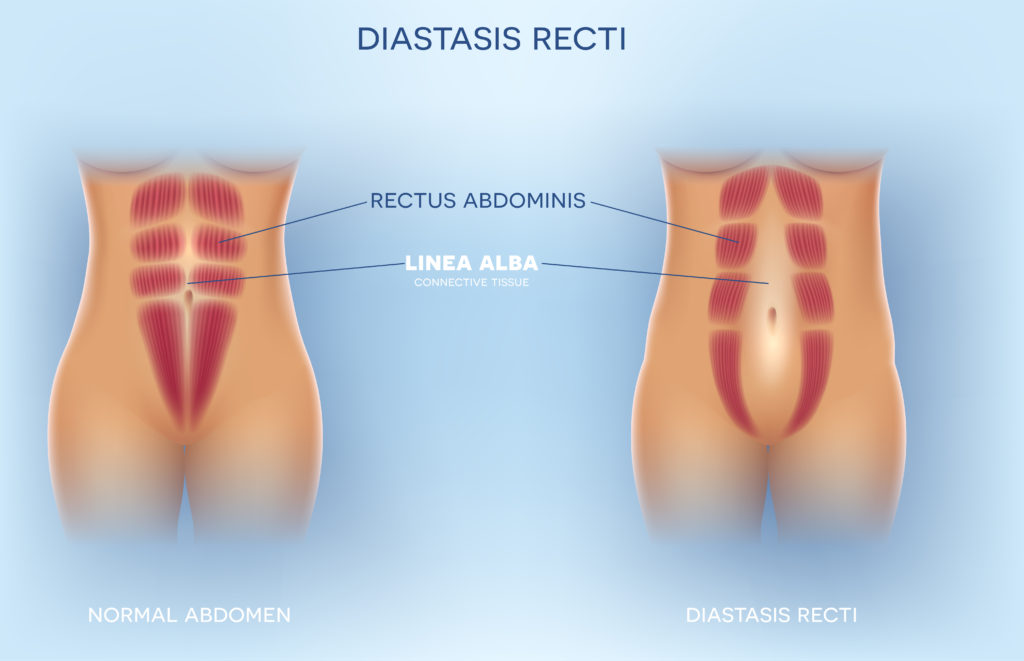
The full medical term for ab separation is Diastasis recti abdominis, or DRA for short. It refers to a separation of the rectus abdominal muscles (the muscles that form a “six pack”) along the midline of the abdomen, or the linea alba. The linea alba is a band of connective tissue to which the left and right abs connect. During pregnancy, fluctuating hormones (such as relaxin progesterone and estrogen), combined with a growing uterus cause the abdominal muscles to stretch, thin out and change shape, and can result in the linea alba being stretched3.
The separation can happen above, around, and/or below the navel, and can be classified as mild, moderate or severe, based on the distance between the ab muscles. There is no single definition in clinical practice of what distance is considered to be diastasis recti, and there are various methods that can be used to measure the gap.
The older and more low-tech way to determine the extent of ab separation is to feel the abdomen and measure the distance between the abs using finger widths (e.g. a distance of 2 or more fingerbreadths either 4.5 cm above, at or 4.5 cm below the bellybutton, can be considered as diastasis recti). Doctors and other healthcare providers may also use tools like measuring tape or ultrasound to get a more accurate measurement.
How Common is Ab Separation?
I remember how shocked I was at age 25, when a close friend of mine described the ab separation that she developed after her difficult first pregnancy. Her doctor was concerned that her baby would arrive early, so she was given steroids to ensure that his lungs were developed enough in case he was born prematurely. This resulted in her baby growing rapidly, and consequently, her ab muscles developed a wide separation in the middle, which lasted for months afterward. At the time, I had never even heard of this condition as a consequence of pregnancy, and I thought it was a rare occurrence, due to the circumstances of her pregnancy.
When in fact, the opposite is true. Most women will have some ab separation during their pregnancy and/or postpartum period. In fact, one study of 84 women pregnant with their first child found that 100% of the women had diastasis recti at 35 weeks of pregnancy1. Another recent study of 229 women found that 82.6% of them had ab separation during the first postpartum year4.
Some women’s bodies may heal naturally after giving birth, and their abs will return to their normal position, but for many women, the ab separation can take months to over 1 year to heal completely. A recent Scandinavian study which looked at 300 pregnant women (with their first child) found that 60.0% still had ab separation at 6 weeks postpartum, 45.4% at 6 months, and 32.6% at 12 months postpartum2.
What are the Risk Factors for Ab Separation?
There are a number of risk factors that have been suggested to contribute to ab separation, such as older maternal age, having previously had babies, c-section, weight gain during pregnancy, high birth weight, multiple pregnancy, and child care5. However, there are still questions on validity of these risk factors. For example, the Scandinavian study I mentioned above found no difference in the prevalence of ab separation based on age, height, weight gain during pregnancy, or caesarean section2. The only risk factor identified in that study was heavy lifting (mothers who did heavy lifting 20 times per week or more were slightly more likely to have ab separation)2. Similarly, a 2009 study found that mother’s age, body mass index (BMI), gestational age, and the duration of labor were not risk factors for developing ab separation3.
So there is still very little known on the actual risk factors for developing ab separation, but in view of the high prevalence of ab separation seen in late pregnancy, I think its safe to say that any pregnancy can lead to diastasis recti.
What are the consequences of Ab Separation?
The main consequence of ab separation is having a visible “pooch” or “mummy tummy”. Since the abs have been thinned out and pulled to the side during pregnancy, they wont be doing a great job at keeping your abdomen “flat”. You may also notice a dome-ing of your abs if you do a sit-up. It can affect the strength of your ab muscles, and how you are able to move your core, and even how you take breaths9.
It has been suggested that diastasis recti can cause some more serious physical problems such as causing instability in the lower back and pelvis resulting in lower back and pelvic girdle pain, and be associated with various pelvic floor dysfunctions such as urinary incontinence, anal incontinence, and pelvic organ prolapse5. In some extreme (and rare) cases, it may also lead to a hernia, if the linea alba tears and internal organs are pushed through the opening, which could require surgery to correct8.
The good news, however, is that a few recent studies have found no association between diastasis recti and pelvic floor dysfunctions such as urinary incontinence and pelvic organ prolapse4,6 or lower back or pelvic pain2. So, although both the pelvic floor muscles and the ab muscles are both greatly affected by pregnancy, there may not be such a strong association between pelvic floor dysfunctions and diastasis recti as previously thought. In fact, one recent study of 300 women found a higher prevalence of pelvic organ prolapse at 6 weeks postpartum in women without diastsis recti (15.9%) as compared to those with diastasis recti (4.1%)6.
How to check if you have Ab Separation
It’s easy to check yourself for ab separation. In the above video, Jen walks you through how you can feel your abs to see if you still have a post-pregnancy ab separation (or follow the steps below).
- Lie on your back with your feet on the floor, in a somewhat neutral position. Try to keep your ribcage on the floor, and keep a small curve in your lower back. Your pelvis (hip bones and pubic bones) are flush.
- Insert your index in your belly button. Lift your head a little, and engage the abs a tiny bit. Walk the fingers upwards from the navel along the midline of the abdominals, and try to feel how deep your fingers sink into your abdomen, and how wide the separation is.
- Repeat the same as you walk your fingers down below your navel.
How can diastasis recti be treated?
Its always a good idea to speak to your doctor, healthcare provider or a physiotherapist to get a professional evaluation and diagnosis of your ab separation, as well as a treatment plan. In some women, no treatment is even needed, as the abs will return to their pre-pregnancy position on their own.
The other good news is that in many cases, ab separation can be treated with targeted ab exercises, at home, with little to no equipment needed. However, not all exercises are appropriate, and it appears that there are some ab exercises that work better than others in helping to close the gap in ab separation.
A recent 2019 study split 40 postpartum women with diastasis recti into two groups: Group A were assigned a deep core stability-strengthening program as well as a traditional abdominal exercise program, and Group B were assigned the traditional abdominal exercise program alone. While both groups succeeded in reducing the gap between their abs, Group A (the deep core stability program) did significantly better than Group B7 at healing their diastasis recti.
The deep core stability program from this study included diaphragmatic breathing, pelvic floor contractions, planks, and isometric abdominal contractions7 . The women attended coaching sessions 3 times a week, for 8 weeks, and were encouraged to repeat the same exercises daily as a home workout.
Strengthening the deep core, and the lower-abdominals in particular, are thought to help heal ab separation by creating a muscular “corset”. There are a number of Pilates moves that can help to engage the deep core and help heal ab separation. It is important that while you are healing from diastasis recti, to go easy on yourself and slowly incorporate gentle and gradual movement and exercise that focuses on breathing, pelvic floor and lower transverse ab engagement. If you see a physiotherapist, they can also perform manual therapy to help bring your abs back together (soft tissue mobilization, myofascial release)10.
In more severe cases of ab separation, when exercise and physiotherapy are not enough to close the gap, surgery ( “abdominoplasty” or “a tummy tuck.”) can be done to bring the abs back together.
I had mild diastasis recti after both of my pregnancies. I was so fortunate that I met my good friend Jen Hodgkinson soon after having my first son (our boys are 1 month apart in age). She is a postnatal movement specialist and Pilates instructor. I took her classes religiously during both of my maternity leaves (hello mom and baby classes!), and I was able to heal my ab separation within about 6 months. I highly recommend her online on-demand Postnatal Pilates and Movement Program . For 12$ per month, you get monthly access to the Postnatal Pilates and Movement Program, PLUS all-access to the Train with Jen On-Demand Library.
What to avoid when you have diastsis recti
When you are postpartum and still have diastasis recti, you should avoid exercises that cause a bulging of the abs, such raising the lower limbs above the ground while lying on the back, abdominal sit-ups and crunches. Straining should also be avoided (such as with constipation) and intense coughing, and lifting heavy objects10. Also try to avoid using your abs to lift your upper body whenever you get up from lying down. It is good practice to roll to your side and use your arms to push yourself up to a seated position.
I hope you have enjoyed my review on ab separation, and I would love to read your comments!
References
1. Fernandes da Mota PG, Pascoal AG, Carita AI, Bø K. Prevalence and risk factors of diastasis recti abdominis from late pregnancy to 6 months postpartum, and relationship with lumbo-pelvic pain. Man Ther. 2015 Feb;20(1):200-5. doi: 10.1016/j.math.2014.09.002. Epub 2014 Sep 19. PMID: 25282439.
2. Sperstad JB, Tennfjord MK, Hilde G, Ellström-Engh M, Bø K. Diastasis recti abdominis during pregnancy and 12 months after childbirth: prevalence, risk factors and report of lumbopelvic pain. Br J Sports Med. 2016 Sep;50(17):1092-6. doi: 10.1136/bjsports-2016-096065. Epub 2016 Jun 20. PMID: 27324871; PMCID: PMC5013086.
3. Rett MT, et al. Prevalence of diastasis of the rectus abdominis muscles immediately postpartum: comparison between primiparae and multiparae. Revista Brasileira de Fisioterapia. 2009;13(4):275–280. doi: 10.1590/S1413-35552009005000037.
4. Fei H, Liu Y, Li M, He J, Liu L, Li J, Wan Y, Li T. The relationship of severity in diastasis recti abdominis and pelvic floor dysfunction: a retrospective cohort study. BMC Womens Health. 2021 Feb 15;21(1):68. doi: 10.1186/s12905-021-01194-8. PMID: 33588826; PMCID: PMC7885475.
5. Gluppe SL, Hilde G, Tennfjord MK, Engh ME, Bø K. Effect of a Postpartum Training Program on the Prevalence of Diastasis Recti Abdominis in Postpartum Primiparous Women: A Randomized Controlled Trial. Phys Ther. 2018 Apr 1;98(4):260-268. doi: 10.1093/ptj/pzy008. PMID: 29351646; PMCID: PMC5963302.
6. Bø K, Hilde G, Tennfjord MK, Sperstad JB, Engh ME. Pelvic floor muscle function, pelvic floor dysfunction and diastasis recti abdominis: Prospective cohort study. Neurourol Urodyn. 2017 Mar;36(3):716-721. doi: 10.1002/nau.23005. Epub 2016 Mar 31. PMID: 27037746.
7. Thabet AA, Alshehri MA. Efficacy of deep core stability exercise program in postpartum women with diastasis recti abdominis: a randomised controlled trial. J Musculoskelet Neuronal Interact. 2019 Mar 1;19(1):62-68. PMID: 30839304; PMCID: PMC6454249.
8. Aguirre, Diego A., et al. “Abdominal wall hernias: imaging features, complications, and diagnostic pitfalls at multi–detector row CT.” Radiographics 25.6 (2005): 1501-1520.
9. Spitznagle TM, Leong FC, Van Dillen LR. Prevalence of diastasis recti abdominis in a urogynecological patient population. Int Urogynecol J Pelvic Floor Dysfunct. 2007;18(3):321–8
10. Michalska A, Rokita W, Wolder D, Pogorzelska J, Kaczmarczyk K. Diastasis recti abdominis – a review of treatment methods. Ginekol Pol. 2018;89(2):97-101. doi: 10.5603/GP.a2018.0016. PMID: 29512814.